- Admin
- #466
Offline
Confirmed deaths, and they say it can take up to 2 weeks to sort it out.I did some more studying of trends late last night, using the Worldometers data, and there are few more things that standout significantly as anomalies.
It is really amazing what can be gleaned once the numbers reach a certain point and trends form, and I can state with a very, very high degree of certainty that these five things are simply not possible, even if you factor in the proverbial death lag:
- Florida has 232,718 cases, but only 4,009 deaths
- Texas has 229,619 cases, but only 2,944 deaths
- Georgia has 103,890 cases, but only 2,922 deaths
- Tennessee has 55,986 cases, but only 685 deaths
- South Carolina has 48,909 cases, but only 884 deaths
Unless most of these states' citizens have different DNA than the rest of the world's, or their populations are remarkably younger (they're not), these numbers are clearly not possible. I am not going to say its intentional, but at a minimal, something is not being tabulated properly.
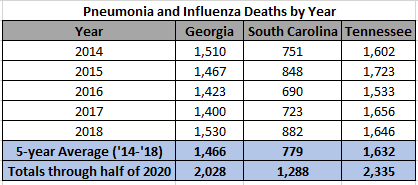
So, with that in mind, I decided to once again take a look at the Pneumonia and Influenza death data. We have already covered Florida and Texas yesterday, so I will now do Georgia, South Carolina, and Tennessee:
So, once again, either COVID deaths are intentionally being labeled as P&I, or we have an absolutely massive Pneumonia/Influenza pandemic on our hands in specific states but not others.
It doesn't take an Epidemiology degree or being a medical expert to figure these things out. All you have to do is be good at math and simple data analytics.
Here are my sources, in case anyone would like to check my work:
United States COVID - Coronavirus Statistics - Worldometer
United States Coronavirus update with statistics and graphs: total and new cases, deaths per day, mortality and recovery rates, current active cases, recoveries, trends and timeline.www.worldometers.info
Provisional Death Counts for Coronavirus Disease 2019 (COVID-19)
National Center for Health Statisticswww.cdc.gov

When you rack up a body count, we may not get perfect data as it is happening.